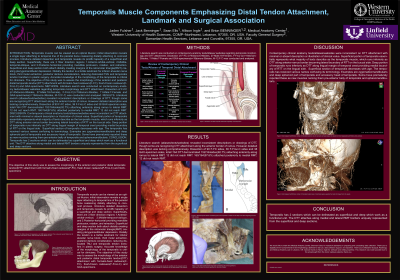
Purpose of the Study: The purpose of this study was to evaluate the morphology and distal tendon attachment (DTT) of the temporalis muscle using formalin-fixed, fresh-frozen, and GAX-prepared cadaver specimens. While contemporary anatomy texts often describe the temporalis as a single-layered muscle, dissection reveals distinct superficial and deep sections with clinical implications. Because the distal tendon serves as a key landmark for nerve blocks, third molar extraction, TMJ reduction, denture design, and tendon transfer procedures, a detailed understanding of its attachments is essential for dental and surgical practice.
Methods: A literature review of anatomy texts, atlases, and online resources was conducted to examine descriptions of temporalis morphology and distal tendon attachment. Anatomical dissections were performed on 45 formalin-fixed cadavers (90 sides; 27 male, 18 female), 18 fresh-frozen cadavers (36 sides; 11 male, 7 female), and 19 GAX-prepared specimens (38 sides; 12 male, 7 female), totaling 164 sides. Each specimen was assessed for anterior and posterior tendon attachment points and findings were compared across cadaver preparation types.
Results: The literature review revealed inconsistent or incomplete descriptions of distal tendon attachments. Dissection of 164 sides demonstrated that 152/164 (92.7%) had anterior attachment along the ramus to the lateral retromolar triangle (RMT), while 12 did not reach the RMT. Posterior attachment to the medial RMT was present in 160/164 (97.6%) specimens, with 12 failing to reach the RMT. These findings confirm that both superficial and deep portions of the temporalis contribute to the margins of the RMT, though anatomical variation was observed.
Conclusion: The temporalis muscle can be divided into superficial and deep sections that function as a unit, with distinct distal tendon attachments forming the medial and lateral borders of the retromolar triangle. Current anatomical references insufficiently describe these details, but accurate recognition of distal tendon morphology is clinically significant for oral surgery, anesthesia, prosthodontics, and temporomandibular procedures. Improved awareness of temporalis structure may enhance surgical accuracy and reduce procedural complications.
Articles: Hwang K, Kim J, Chung IH. Clinical importance of morphology and nomenclature of distal attachment of temporalis tendon. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(6):719-724. doi:10.1016/j.tripleo.2011.06.024. Schon-Ybarra MA, Martinez L, Martinez F. Medial portion of M. temporalis and its potential involvement in facial pain. Clin Anat. 2001;14(1):47-52. doi:10.1002/1098-2353(200101)14:1 < 47::AID-CA1006>3.0.CO;2-V.
Books: Standring S, ed. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. London, UK: Elsevier; 2021. Abrahams P, Craven JL, Lumley JSP. Illustrated Clinical Anatomy. 2nd ed. London, UK: Hodder Arnold; 2011. Berkovitz BKB, Moxham BJ, Linden RW. Head and Neck Anatomy: A Clinical Reference. Boca Raton, FL: CRC Press; 2016. Chung KW, Chung HM. Gross Anatomy. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011. Ellis H. Clinical Anatomy: A Revision and Applied Anatomy for Clinical Students. 12th ed. Chichester, UK: Wiley-Blackwell; 2018. Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 7th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2014.